Prison Health Care Quality Monitoring Systems Vary by State
How jurisdictions can select the best way to measure performance

In this June 1, 2017 photo, Verdia Miller stands with a cane she has to use at the Chillicothe Correctional Center in Chillicothe, Mo. In Missouri, the number of people age 50 and older who are in prison is increasing at 11 times the rate of the prison population overall.
Meg Vatterott/Missourian/APThis is the eighth analysis in a series examining how health care is funded and delivered in state-run prisons, as well as how care continuity is facilitated upon release.
Health care delivered to incarcerated individuals has far-reaching implications, so monitoring its quality is an important element of high-performing correctional systems.
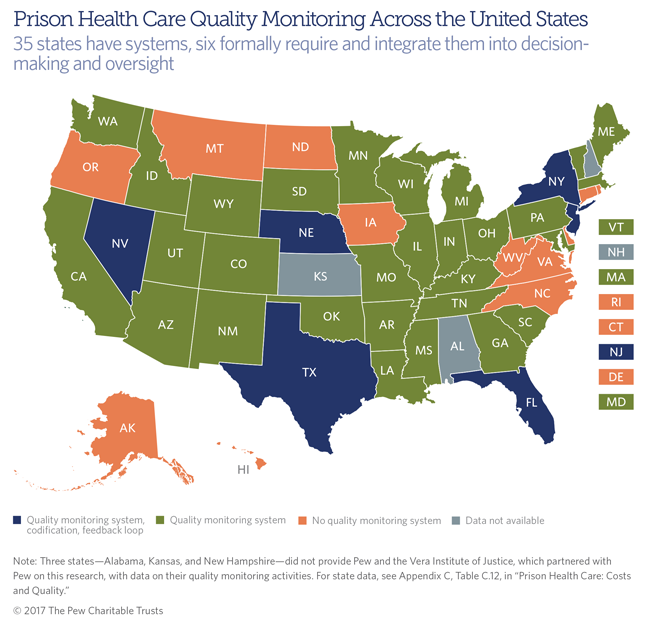
A first-of-its-kind report by The Pew Charitable Trusts details whether and how states monitor the quality of care they provide in prison. Thirty-five states reported that they operated a prison health care quality monitoring system in fiscal year 2016. Six—Florida, Nebraska, Nevada, New Jersey, New York, and Texas—indicated that they formally require quality monitoring and build in regular opportunities to incorporate the findings into decision-making and legislative oversight.
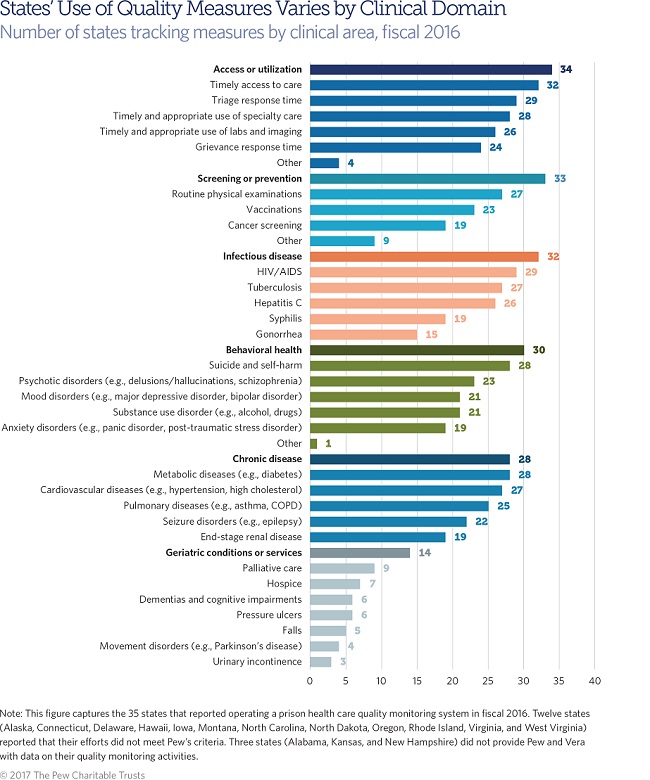
To gain insight into what those 35 states measured, researchers asked departments of correction whether their monitoring covered one or more of six clinical domains:
|
|
|
|
|
|
Two-thirds of the states with systems (24 out of 35) reported covering every domain except for geriatric conditions or services; just 14 states monitored that domain. Twelve states (Arizona, Georgia, Indiana, Louisiana, Maryland, Massachusetts, Michigan, Minnesota, Nebraska, New Jersey, New York, and Utah) reported monitoring every domain. Florida’s system incorporated the fewest: only one, screening and prevention.
States without a quality monitoring system reported engaging in a wide range of related activities, including regular audits of practices and protocols, inmate grievance investigations, and mortality reviews. But a majority agreed or strongly agreed that establishing a system is necessary to achieve at least an adequate level of quality, would improve the quality of care provided, and would improve states’ understanding of the value of their prison health care spending.
How should state prisons select measures to monitor?
Researchers at the RAND Corp., working with a panel of clinical experts in 2009, identified a set of measures they argued were most suitable for prison health care. Besides the measures recommended, which provide a useful reference point, the process researchers used may be instructive for prison health care practitioners seeking to launch or bolster their quality monitoring systems.
First, hundreds of measures from public sources were screened for relevance to primary care and prison populations, which have high rates of infectious or chronic disease, mental illness, and substance use disorder. Selected measures were then judged against four criteria: importance, scientific soundness, workability, and likelihood of producing interpretable results.
Measures meeting most or all of these requirements were rated based on validity and feasibility. Valid measures were grounded in scientific evidence or professional consensus; linked to care with identifiable health benefits; indicative of higher quality with higher adherence; and associated with results that were reasonably under the control of providers. Measures were feasible if adherence data were accessible or soon to be accessible; estimates of adherence would be reliable and unbiased; and failure to document adherence would be an inherent sign of poor quality.
RAND Corp. Criteria for Evaluating Measures
| Importance |
|
| Scientific Soundness |
|
| Workability |
|
| Interpretability |
|
Panelists agreed on two broad recommendations. First, they favored a mix of explicit and implicit measures. Explicit measures are quantitative in nature (for example, the percentage of inmates who received a physical examination within the first week of incarceration), with clear parameters, such as time frames and diagnostic codes. Implicit measures are qualitative and based on clinical judgments about the adequacy or appropriateness of delivered care (for instance, a peer review or mortality review). Panelists agreed that implicit measures help detect errors or deficiencies that are difficult to quantify. Second, they argued that measures and monitoring systems need to be used alongside quality improvement programs that trigger action in response to identified weaknesses.
Every state must tailor its prison health care quality monitoring system—if it has one—to its unique circumstances and objectives. But the process used by this esteemed panel with deep and broad expertise offers an adaptable model for deciding what to monitor and how to do it.
Matt McKillop leads The Pew Charitable Trusts’ research on state and local correctional health care.







