Trends in U.S. Antibiotic Use
New data needed to improve prescribing, combat threat of antibiotic resistance

A drug-resistant strain of Salmonella as viewed through a microscope.
CDC/Science Source
This issue brief was updated Aug. 30, 2018, to clarify the conclusions.
Overview
Antibiotic resistance is a pressing global public health problem. This first report on trends in antibiotic use in the United States brings together diverse sources of information in both human health care and animal agriculture settings. It complements and informs efforts to set evidence-based goals aimed at reducing unnecessary antibiotic use. Lowering the use of these drugs will slow the emergence of resistance. While today’s data are not perfect, this report begins to establish a baseline and outlines areas where better information is needed. More comprehensive data would allow policymakers to refine priorities, target interventions, and track progress over time.
Antibiotic use in health care
The U.S. has a relatively high antibiotic prescribing rate. For example, an analysis of 2004 outpatient data from the U.S. and 27 European countries found the U.S. had the fourth-highest rate.1 Although data are incomplete, existing evidence suggests that a significant portion of antibiotic use across U.S. health care settings is inappropriate—from primary care offices and emergency rooms to hospitals and long-term care facilities. Policy options and incentives will vary depending on the setting, but enhanced data are needed across all settings in order to design targeted and effective stewardship interventions that will improve the use and preserve the effectiveness of this valuable resource.
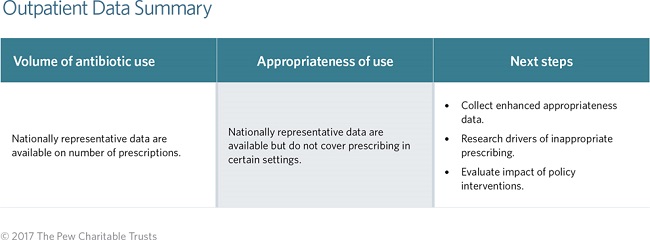
Antibiotic use in outpatient care
Volume of use
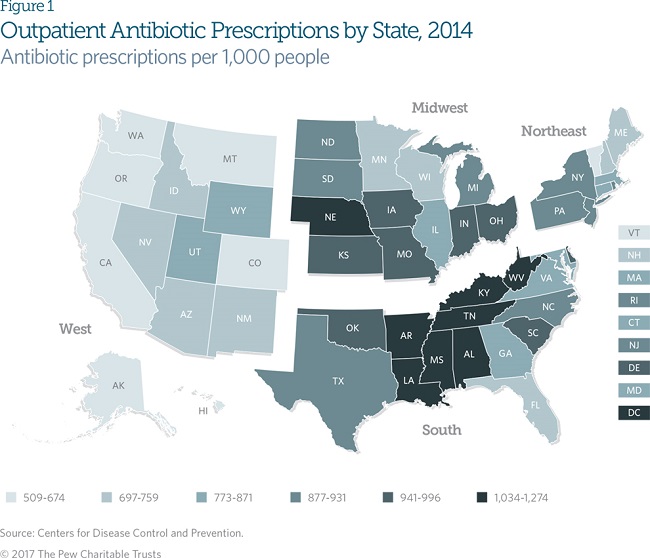
The overall antibiotic prescribing rates for doctors’ offices, emergency departments, and other outpatient settings in the U.S. have decreased in recent years but remain high by international standards. In 2014, for example, outpatient health care providers in the United States wrote over 266 million antibiotic prescriptions, amounting to 835 antibiotic prescriptions for every 1,000 people.2 While that represents a 6 percent decline since 2006,3 this figure was more than 2½ times Sweden’s rate in the same year: 328 prescriptions for every 1,000 people.4 U.S. prescribing rates vary by state, with numbers generally higher in Southern states and lowest in the West.5 (See Figure 1.) Although geographic variation does not clearly indicate differences in the appropriateness of prescribing, it suggests that targeted stewardship has the potential to reduce overall rates of antibiotic use in the U.S. Further research is needed to identify the clinical, socioeconomic, demographic, and other factors driving inappropriate antibiotic use.
Antibiotic prescribing trends vary widely by provider type. For example, prescribing rates for primary care doctors fell by 15 percent from 2011 to 2014, while those for nurse practitioners and physician assistants rose 41 percent.6 The latter figure does not take into account possible changes in patient caseloads—for instance, whether providers are seeing more patients with bacterial infections. However, such differences in trends highlight the importance of implementing comprehensive stewardship initiatives that are directed at all providers. Further research on the drivers behind varied prescribing rates—such as regional variations in patients’ expectations around antibiotic therapy; the availability of education and guidance about antibiotic use and resistance for different providers; economic considerations that influence prescribing practices; and other factors—would furnish important information to help shape targeted antibiotic stewardship efforts.
Appropriateness of use
At least 30 percent of oral antibiotics prescribed in U.S. outpatient settings are unnecessary.7 Of the total excess prescriptions, nearly three-quarters are for acute respiratory conditions, including asthma, allergies, colds, and other infections not caused by bacteria, which therefore do not respond to antibiotics.

In cases where an antibiotic is necessary to treat an infection, it is important to prescribe the appropriate drug. An examination of antibiotic prescribing for three common respiratory conditions found that in about a third of cases, providers selected the wrong drug.8 Choosing an antibiotic that targets only the bacteria most likely to cause a given illness could substantially reduce the development of resistance.9
The three respiratory conditions included in the above study accounted for nearly 30 percent of all antibiotic prescriptions in outpatient settings. Additional data are needed to assess the appropriateness of antibiotic selection for other common conditions managed in such settings.
Improving data
There are many areas where adequate data on outpatient antibiotic prescribing are lacking. For example, prescribing in retail and urgent care clinics, in dental offices, or via telemedicine is not currently captured. Better data and qualitative research on the drivers of antibiotic use would enable public health agencies, the health care industry, professional societies, and other stakeholders to implement interventions that could improve the appropriateness of prescribing.
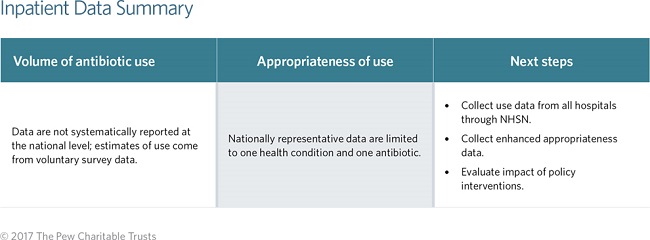
Antibiotic use in inpatient care
Volume of use
Over half of all hospital patients receive antibiotics during their stay—a figure unchanged in recent years.10 However, while the overall rate of hospital antibiotic use has remained steady, the mix of drugs being used has changed. Between 2006 and 2012 specifically, the use of many broad-spectrum antibiotics increased, with a commensurate decrease in use of many narrow-spectrum antibiotics that target a limited group of bacteria.11 As broad-spectrum antibiotics have been shown to significantly increase the risk of drug-resistant infections, this trend is concerning.12

Appropriateness of use
Unfortunately, the U.S. lacks comprehensive data on the appropriateness of inpatient antibiotic use.13 Existing research suggests that improvement is needed. For example, one study examining the treatment of a common bacterial condition (urinary tract infection) and use of a commonly prescribed antibiotic (vancomycin) in a sample of hospitals across the country found that 37 percent of prescriptions were potentially unnecessary or inappropriate (written for the wrong duration or antibiotic).14 In order to have a more complete assessment of the appropriateness of antibiotic use in U.S. hospitals, additional data that capture more conditions and drugs are needed.
Improving data
The Centers for Disease Control and Prevention has the capacity to track hospital antibiotic use through its National Healthcare Safety Network (NHSN), but currently data reporting is voluntary and limited. As of March 2016, only a small fraction of hospitals report their antibiotic use.15 Mandatory reporting would provide the data needed to establish a more accurate baseline of current use, identify where and what types of stewardship interventions would be most effective, and measure progress toward reducing inappropriate prescribing.
Antibiotic use in animal agriculture
Antibiotics are used in animal agriculture to treat, control, and prevent disease. Currently, little information is publicly available on the volume or appropriateness of that use in the U.S. Experiences in other countries—for instance, through the Monitoring of Antimicrobial Resistance and Antibiotic Usage in Animals in the Netherlands (MARAN) or the European Surveillance of Veterinary Antimicrobial Consumption projects—demonstrate the feasibility and value of collecting data to better understand antibiotic use on farms.16 Collecting such data in the U.S. will be key to establishing a current baseline of use; identifying opportunities to responsibly reduce antibiotic use; setting evidence-based reduction goals; and measuring progress over time.
Collecting nationally representative use data is complicated by the diversity of how industries are structured. For example, the poultry industry is highly integrated whereas the cattle industry is more fragmented, resulting in differences across species in the use of centralized data collection systems.17 Nonetheless, as other countries have demonstrated, enhanced data collection is possible.
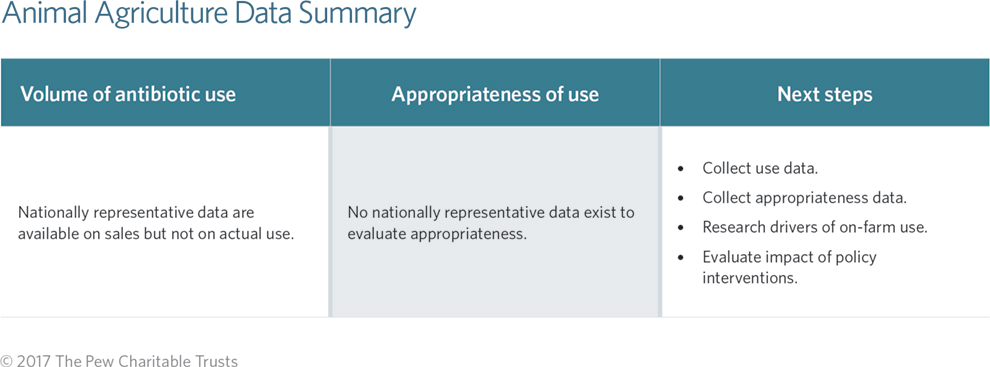
Volume of use
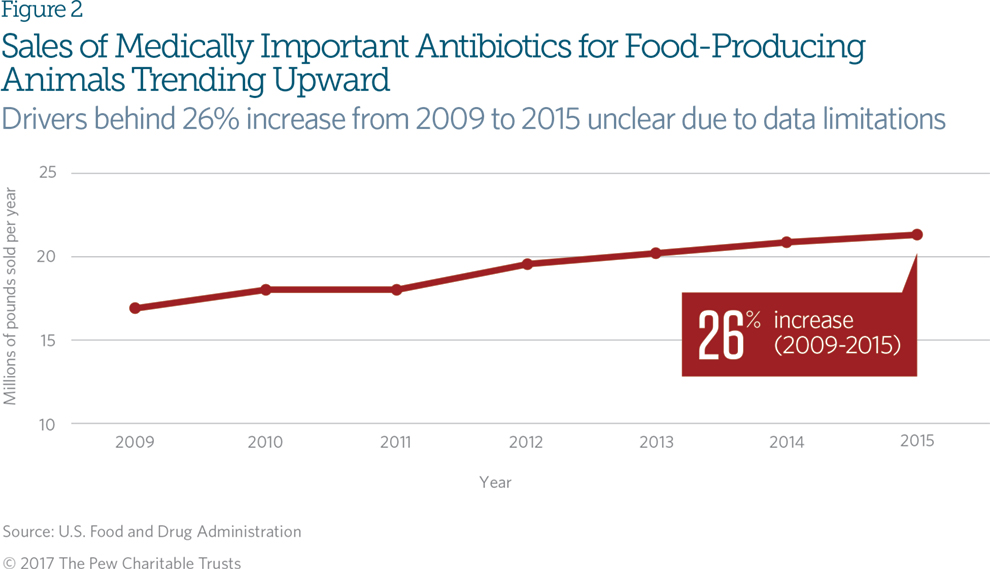
The only national estimates of total antibiotic use in U.S. food animal production come from sales data, which can provide insights into trends in use. In 2015, the last year for which data are available, approximately 9.7 million kilograms, or 21.4 million pounds, of antibiotics considered important for human use were sold for use in animal agriculture, a 26 percent total increase over 2009 sales.18 (See Figure 2.) The reason for this increase cannot be determined from available data because sales information does not capture insights on how the drugs were used. Current data also do not break out antibiotic sales by animal species.19 All of these limitations point to the need for additional information to better understand why the sales are trending upward.
Appropriateness of use
National data to evaluate the appropriateness of antibiotic use in animal agriculture are limited. The U.S. Department of Agriculture (USDA) collects nationally representative survey data on animal health, management practices, and productivity. However, the data are collected infrequently (about every five years), and surveys differ widely across species.20 Additional limitations include insufficient quantitative information on reasons for use, and specific drugs, dosages, and duration.21 Without such information, it is difficult to determine why antibiotics are used in U.S. animal agriculture, which uses are appropriate, and where alternatives to antibiotics might be used.
Improving data
Expanding the USDA’s existing survey to include more detailed questions about the volume of actual use and the dosages, duration, and conditions for which antibiotics are being used would provide the missing information about antibiotic use on farms. This would enable stakeholders to evaluate the impact of recent policy changes, monitor trends, and identify opportunities to improve antibiotic use.
Conclusion
Currently available data on antibiotic use in the U.S. are insufficient. Key stakeholders from the public, private, and nonprofit sectors must work together to improve the quality and availability of data in order to expand antibiotic stewardship in human health care and promote the responsible use of these drugs in food animals. To improve antibiotic use data:
- The Centers for Medicare & Medicaid Services should require mandatory reporting of hospital antibiotic use to the National Healthcare Safety Network.
- Congress should support the USDA’s and Food and Drug Administration’s capacity to implement currently underfunded data collection plans through an increase in appropriations.
- Livestock producers, retailers, and researchers should collaborate to determine how best to enhance data collection on the farm. Pew will continue to work with various partners to improve the quality and quantity of antibiotic use data on all fronts, and will periodically evaluate progress and remaining gaps.
Endnotes
- Herman Goossens et al., “Comparison of Outpatient Systemic Antibacterial Use in 2004 in the United States and 27 European Countries,” Clinical Infectious Diseases 44 (2007): 1091–95, doi:10.1086/512810.
- Centers for Disease Control and Prevention, “Outpatient Antibiotic Prescriptions—United States, 2014,” accessed Dec. 12, 2016, https://www.cdc.gov/getsmart/community/pdfs/annual-reportsummary_2014.pdf.
- Katie J. Suda et al., “Trends and Seasonal Variation in Outpatient Antibiotic Prescription Rates in the United States, 2006 to 2010,” Antimicrobial Agents and Chemotherapy 58, no. 5 (2014): 2763–66, doi:10.1128/AAC.02239-13; Centers for Disease Control and Prevention, “Outpatient Antibiotic Prescriptions—United States, 2014.”
- Public Health Agency of Sweden and National Veterinary Institute, SWEDRES|SVARM 2014: Consumption of Antibiotics and Occurrence of Antibiotic Resistance in Sweden (2014), http://www.sva.se/globalassets/redesign2011/pdf/om_sva/publikationer/ swedres_svarm2014.pdf.
- Centers for Disease Control and Prevention, “Outpatient Antibiotic Prescriptions—United States, 2014.”
- Centers for Disease Control and Prevention, “Outpatient Antibiotic Prescriptions—United States, 2014.”; Centers for Disease Control and Prevention, “Outpatient Antibiotic Prescriptions—United States, 2011,” accessed Dec. 12, 2016, https://www.cdc.gov/getsmart/community/pdfs/annual-reportsummary_2011.pdf.
- Katherine E. Fleming-Dutra et al., “Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010-2011,” Journal of the American Medical Association 315, no. 17 (2016): 1864–73, doi:10.1001/jama.2016.4151.
- Adam L. Hersh et al., “Frequency of First-Line Antibiotic Selection Among US Ambulatory Care Visits for Otitis Media, Sinusitis, and Pharyngitis,” JAMA Internal Medicine 176, no. 12 (2016): 1870–72, doi:10.1001/jamainternmed.2016.6625.
- Public Health England, Management of Infection Guidance for Primary Care for Consultation and Local Adaptation (May 2016), accessed Nov. 16, 2016, https://www.gov.uk/government/uploads/system/uploads/attachment_data/ file/524984/Management_of_infection_guidance_for_primary_care_for_ consultation_and_local_adaptation.pdf; Matthew E. Falagas and Petros Kopterides, “Risk Factors for the Isolation of Multi-Drug-Resistant Acinetobacter baumannii and Pseudomonas aeruginosa: A Systematic Review of the Literature,” The Journal of Hospital Infection 64, no. 1 (2006): 7–15, doi:10.1016/j.jhin.2006.04.015; Balázs Ivády et al., “Factors Influencing Antimicrobial Resistance and Outcome of Gram-Negative Bloodstream Infections in Children,” Infection 44, no. 3 (2016): 309–321, doi:10.1007/ s15010-015-0857-8; G. Gopal Rao, “Risk Factors for the Spread of Antibiotic-Resistant Bacteria,” Drugs 55, no.3 (1998): 323–330, doi:10.2165/00003495-199855030-00001.
- James Baggs et al., “Estimating National Trends in Inpatient Antibiotic Use Among US Hospitals From 2006 to 2012,” JAMA Internal Medicine 176, no. 11 (2016): 1639–48, doi:10.1001/jamainternmed2016.5651.
- Ibid.
- Public Health England, Management of Infection Guidance for Primary Care for Consultation and Local Adaptation (May 2016), https://www.gov.uk/government/uploads/system/uploads/attachment_data/ file/524984/ Management_of_infection_guidance_for_primary_care_for_consultation_and_ local_adaptation.pdf; Matthew E. Falagas and Petros Kopterides, “Risk Factors for the Isolation of Multi-DrugResistant Acinetobacter baumannii and Pseudomonas aeruginosa: A Systematic Review of the Literature,” The Journal of Hospital Infection 64, no. 1 (2006): 7–15, doi:10.1016/j.jhin.2006.04.015; Balázs Ivády et al., “Factors Influencing Antimicrobial Resistance and Outcome of Gram-Negative Bloodstream Infections in Children,” Infection 44, no. 3 (2016): 309–321, doi:10.1007/s15010-015-0857-8; G. Gopal Rao, “Risk Factors for the Spread of Antibiotic-Resistant Bacteria,” Drugs 55, no. 3 (1998): 323–30, doi:10.2165/00003495-199855030- 00001.
- Lori A. Pollack et al., “Antibiotic Stewardship Programs in U.S. Acute Care Hospitals: Findings From the 2014 National Healthcare Safety Network Annual Hospital Survey,” Clinical Infectious Diseases 63, no. 4 (2016): 443–49, doi:10.1093/cid/ciw323. Many individual hospitals track antibiotic use in their own facilities as part of their stewardship efforts, and then analyze that data to evaluate appropriateness of antibiotic use.
- Scott Fridkin et al., “Vital Signs: Improving Antibiotic Use Among Hospitalized Patients,” Morbidity and Mortality Weekly Report 63, no. 9 (2014): 194–200, https://www.cdc.gov/mmwr/pdf/wk/mm6309.pdf.
- Presidential Advisory Council on Combating Antibiotic-Resistant Bacteria, Initial Assessments of the National Action Plan for Combating Antibiotic-Resistant Bacteria (March 2016), http://www.hhs.gov/sites/default/files/paccarb-final-report-03312016.pdf. The Centers for Medicare & Medicaid Services is considering mandatory reporting of antibiotic use into the National Healthcare Safety Network.
- “Detailed Info—Fattening Pigs,” Wageningen University & Research, accessed Feb. 7, 2017, http://www.wur.nl/en/Research-Results/Projects-and-programmes/MARAN-Antibiotic-usage/Trends-in-use-per-species/Antibiotic-usage-in-pigs/Detailed-info-fattening-pigs.htm; European Medicines Agency, “Report on ESVAC Trial for Collecting Data on Consumption of Antimicrobial Agents in Pigs” (May 20, 2016), http://www.ema.europa.eu/docs /en_GB/document_library/Report/2016/05/WC500206990.pdf.
- William D. McBride and Kenneth Mathews Jr., “The Diverse Structure and Organization of U.S. Beef Cow-Calf Farms,” ERS Report Summary, U.S. Department of Agriculture (March 2011), https://www.ers.usda.gov/webdocs/publications/eib73/ 7611_eib73.pdf?v=41063; U.S. Department of Agriculture, “Highlights of Structure of the U.S. Poultry Industry, 2010,” APHIS Info Sheet (November 2011), https://www.aphis.usda.gov/animal_health/ nahms/poultry/ downloads/poultry10/Poultry10_is_Structure_highlights.pdf; U.S. Department of Agriculture, Poultry Industry Manual (March 2013), http://www.cfsph.iastate.edu/pdf/fad-prep-nahems-poultry-industry-manual.
- Food and Drug Administration, 2015 Summary Report on Antimicrobials Sold or Distributed for Use in Food-Producing Animals (December 2016), accessed Feb. 7, 2017, http://www.fda.gov/downloads/ForIndustry/UserFees/ AnimalDrugUserFeeActADUFA/UCM534243.pdf.
- Final rule, 81 Fed. Reg. 29129 (May 11, 2016), https://www.gpo.gov/fdsys/ pkg/FR-2016-05-11/pdf/2016-11082.pdf. Species-specific sales data estimates will be included in Animal Drug User Fee Amendments data for 2016.
- U.S. Department of Agriculture, “Collecting Vital Information on Animal Health” (April 2010), https://www.aphis.usda.gov/animal_health/nahms/downloads/ NAHMS_brochure.pdf; Notice, 81 Fed. Reg. 45450 (July 14, 2016), https://www.gpo.gov/fdsys/pkg/FR-2016-07-14/pdf/2016-16612.pdf. The USDA announced a plan to expand the National Animal Health Monitoring System to collect annual antibiotic use data for swine and feedlot cattle.
- U.S. Department of Agriculture, “Proposed Initiatives From the USDA Antimicrobial Resistance Action Plan,” APHIS Info Sheet (April 2015), https://www.aphis.usda.gov/animal_health/nahms/amr/downloads/ ProposedInitiatives.pdf. The USDA’s Agricultural and Resource Management Survey also includes some questions on antibiotic use, but the data provide no information on the drivers or details of such use. Selected National Antimicrobial Resistance Monitoring System (NARMS) studies have collected information on antibiotic use and resistance on study farms. NARMS is operated jointly by the USDA, the Centers for Disease Control and Prevention, and the U.S. Food and Drug Administration to monitor trends in antimicrobial resistance. However, NARMS surveys have relatively small sample sizes and other limitations that impede the system’s ability to provide information that can be used to evaluate the appropriateness of antibiotic use in animal agriculture.


Antibiotic Resistance: When Drugs Don’t Work Anymore
Episode 15

Antibiotic Prescribing Trends in U.S. Raise Flags
Efforts needed to curb the use of broad-spectrum drugs, slow the spread of resistance

FDA Ramps Up Required Animal Antibiotics Data
New rule mandates more comprehensive reporting of drugs sold for use in farm animals
ADDITIONAL RESOURCES




