Is Health Impact Assessment Effective in Bringing Community Perspectives to Public Decision-Making?
Lessons from 4 case studies in California

© Getty Images
Overview
By incorporating health considerations and community viewpoints into the process of evaluating and implementing projects, policies, and programs, health impact assessments (HIAs) can improve public health and expand the use of evidence in decision-making across public sectors. With funding from The California Endowment, the Health Impact Project—a collaboration of the Robert Wood Johnson Foundation and The Pew Charitable Trusts—has supported nine HIAs in California through three separate calls for proposals.
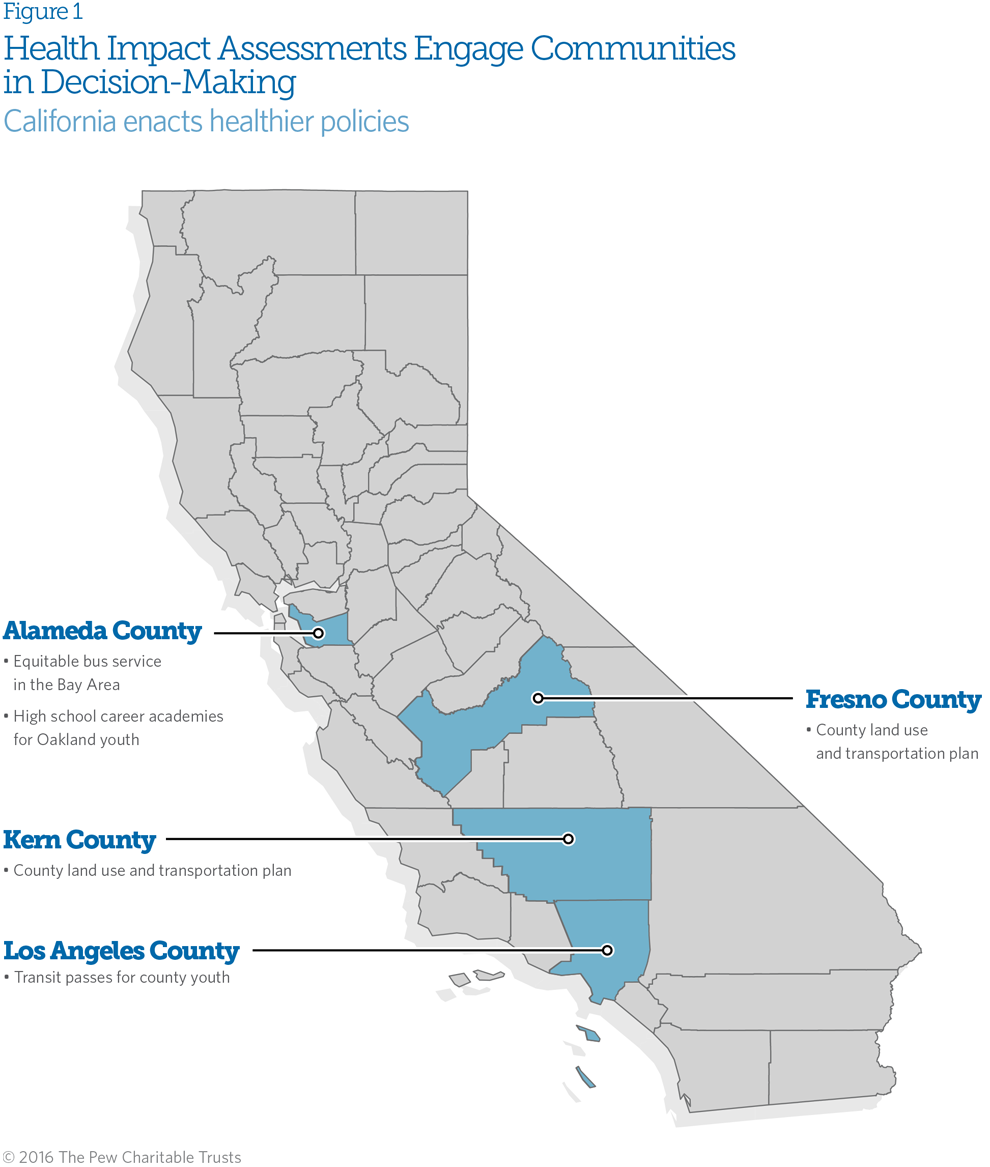
Awardees received up to $250,000 and access to technical assistance and training from the Health Impact Project and a consultant. The HIAs further The California Endowment’s interests in the development of land-use, transportation, and community development policies that promote health in California communities. This brief presents four evaluated case studies examining five of the HIAs—in Kern, Fresno, Los Angeles, and Alameda counties and the city of Oakland. The Health Impact Project conducted interviews with community stakeholders and HIA team members to evaluate the assessments, identify common themes, and develop the case studies. (See “Methods” on Page 15 for more information.) The evaluation sought to answer how and to what extent:
- The HIAs advanced land-use, transportation, and development practices as mechanisms to promote community health.
- The HIA process brought community voices into public decision-making.
- The HIAs helped policymakers better understand how proposals would affect the health of the communities they serve.
- The HIA process identified and led to the adoption of recommendations to maximize potential health benefits and mitigate negative consequences of a proposed action.
- Providing agencies, organizations, and communities with HIA training and opportunities to work with and learn from practitioners increased awareness of and capacity for HIA in California.
The key findings that emerged from the analysis highlight the HIAs’ impacts on relationships within and across agencies and communities and on decision-making, and the challenges and successes that practitioners have faced while conducting these studies. Specifically, the evaluation found that:
- Realizing the benefits of cross-sector collaboration requires strong, committed leadership and a skilled, dedicated team able to manage relationships, support diverse priorities, and engage stakeholders.
- Disseminating the HIA findings and recommendations in a compelling, accessible manner helped to highlight the connections between the decisions being assessed and the effects on health. In the instances where the HIAs were successful with such communication, decision-makers were driven to take appropriate actions.
- Conducting an effective HIA requires appropriate capacity and expertise, and the many challenges and benefits that practitioners experience in engaging community members require different types of support. In particular, the HIA team may require access to experts in HIA process, research methods, public health, and the relevant sectors; sufficient financial, data, and other resources; and cross-sector and multiagency and organizational relationships.
This brief examines these lessons and other findings of the evaluation to provide a clear picture of the strategies that support stakeholder engagement in HIA and the challenges that attend it.
What Is a Health Impact Assessment?
HIA is a rapidly growing field that can help decision-makers make better choices by bringing together scientific data, health expertise, and public input to identify the potential and often overlooked effects, both positive and negative, of proposed laws, regulations, projects, policies, and programs on public health.* Federal, state, and local organizations are increasingly using HIAs to inform decision-making in a range of sectors.†
HIAs broadly take into account environmental, social, and economic factors related to health and evaluate the potential impacts of a proposed project, plan, program, or policy on the health and well-being of the community, including the full range of potential positive and negative effects. HIAs employ a variety of data sources, comprising qualitative and quantitative analysis and input from stakeholders, to identify health concerns related to the proposal and to determine how these impacts may be distributed among the population, especially for groups already at higher risk, such as seniors, children, and low-income families. Finally, HIAs provide pragmatic, evidence-based recommendations about how to reduce risks, promote benefits, and monitor the health effects of the implemented decision.‡
The HIA practitioners define the scope of the factors considered with input from the communities that are likely to be affected by the proposed action and from other relevant stakeholders and decision-makers. A core tenet of HIA is to engage stakeholders throughout the process by bringing residents, decision-makers, business interests, and others together to inform the scope, analysis, and recommendations.
The HIA process
Step 1: Screening. The HIA team and stakeholders determine whether an HIA is needed, can be accomplished in a timely manner, and would add value to the decision-making process.
Step 2: Scoping. The HIA team and stakeholders identify the potential health effects that will be considered and develop a plan for completing the assessment, including specifying their respective roles and responsibilities.
Step 3: Assessment. The HIA team evaluates the proposed project, program, policy, or plan and identifies its most likely health effects using a range of data sources, analytic methods, and stakeholder input to answer the research questions developed during scoping.
Step 4: Recommendations. The team and stakeholders develop practical solutions that can be implemented within the political, economic, or technical limitations of the project or policy to minimize identified health risks and to maximize potential health benefits.
Step 5: Reporting. This step involves dissemination of information—including the HIA’s purpose, process, findings, and recommendations—to a wide range of stakeholders.
Step 6: Monitoring and evaluation. The team and stakeholders evaluate the HIA according to accepted standards of practice. They also monitor and measure its impact on decision-making and health.
HIAs can be fairly quick, using a “rapid” or “desktop” model, or they can take a longer, more comprehensive approach. Rapid HIAs can be completed in weeks or months. They allow consideration of health factors in decision-making—while retaining an emphasis on stakeholder engagement and equity—in cases of compressed timelines, limited resources, or smaller scope of analysis.§ Full-scale HIAs can take between several months and more than a year to complete and often involve a series of public meetings, extensive stakeholder consultation, and collection of new data.||
By helping stakeholders recognize the trade-offs inherent in a proposed action, HIAs ensure that officials and policymakers have the best health information to guide their decisions.
* Health Impact Project, “About Health Impact Assessment,” accessed June 27, 2016, //www.pewtrusts.org/en/projects/health-impact-project/health-impact-assessment.
† Health Impact Project, “Health Impact Assessments in the United States,” accessed June 27, 2016, //www.pewtrusts.org/en/multimedia/data-visualizations/2015/hia-map.
‡ Ibid; and National Research Council, Improving Health in the United States: The Role of Health Impact Assessment (Washington: National Academies Press, 2011), 5, http://www.nap.edu/catalog.php?record_id=13229.
§ As defined by the World Health Organization, equity in health is “the absence of avoidable or remediable differences among groups of people, whether those groups are defined socially, economically, demographically, or geographically.” World Health Organization, “Equity,” accessed Aug. 9, 2016, http://www.who.int/healthsystems/topics/equity/en.
|| National Research Council, Improving Health in the United States.
Community coalitions in Fresno and Kern counties
Residents of Fresno and Kern counties in California’s San Joaquin Valley have some of the nation’s highest rates of concentrated poverty, which is a well-documented risk factor for illness and premature death.1 The region also has some of the highest levels of air pollution and rates of asthma in the state.2 Studies have shown that exposure to air pollution can lead to elevated rates of respiratory disease, such as asthma and bronchitis, and to increased hospital visits.3
A collaborative team of California-based organizations conducted two HIAs to inform transportation and land-use plans that were part of a larger sustainable community strategy (SCS) for the two counties. The team included:
- California Rural Legal Assistance Inc., a nonprofit established 50 years ago to provide legal services to lowresourced rural communities in the state.
- Leadership Counsel for Justice and Accountability, a group created to support low-income, rural communities and increase their access to decision-making.
- Central Valley Health Policy Institute, a publicly funded institution established in 2002 as part of the California State University, Fresno to improve health equity and access to health care in the region.4
- University of California, Davis Center for Regional Change, an advocacy and research department launched in 2007 to support the development of healthy, equitable, and sustainable regions in the state and across the U.S.
- PolicyLink, a national research and action institute advancing economic and social equity.
California S.B. 375, the Sustainable Communities and Climate Protection Act of 2008, “supports the state’s climate action goals to reduce greenhouse gas emissions through coordinated transportation and land-use planning with the goal of more sustainable communities.”5 Under the law, metropolitan planning organizations are required to develop and implement an SCS as part of their regional transportation plans, which must include strategies for transportation, land use, and housing to achieve regional emission targets.6 The HIA team intentionally included community members from both counties in the process, especially low-income residents and those from the highest-poverty areas. The team ensured that these stakeholders had input on the HIA scope and priorities by having them serve on the advisory committee and inviting them to learn more about the law and HIA process at community workshops.
The HIAs examined how the SCSs could potentially affect the accessibility of public transportation and in turn, access to jobs, health care, and schools in each county. The team reviewed published literature and existing data from the U.S. Census Bureau’s American Community Survey to understand the counties’ demographics. It also considered information on public transit routes and schedules to analyze current transportation accessibility.
Community stakeholders stayed engaged throughout the SCS decision-making process. The HIA team’s analysis revealed that Fresno and Kern counties have growing Latino and Asian populations and a disproportionate number of low-income residents and people of color, compared with surrounding counties. From the beginning of the process, the team recognized that these communities face language, resource, and other barriers to participation in public processes. To address this problem, the HIA team specifically tried to make educational meetings and workshops accessible to these residents, invited them to share the HIA findings at public hearings, and reduced barriers to participation by providing translation services and communicating the data and bill language in a way that was accessible to all participants. This strategy not only encouraged community engagement, but it also empowered residents to speak on their own behalf directly with decision-makers. The consistent presence of community members at meetings and the stories they shared gave public officials the opportunity to learn more about the needs and perspectives of their constituents.
HIA recommendations
Based on the findings, the team developed recommendations to promote equity in each county, including to identify the transportation needs of socio-economically disadvantaged communities of color and to invest in those areas to address such issues as gaps in transit service and inadequate sidewalk infrastructure before prioritizing future development. Both the Fresno and Kern councils of governments incorporated recommendations from the respective HIAs into their SCS plans, including:
- Training county staff to assess and consider the potential health impacts of various land-use and transportation scenarios for future decisions.
- Conducting a needs assessment in Fresno County to examine transportation deficiencies and related health outcomes and use the resulting data to prioritize funding and create an action plan.
- Creating a grant program in Fresno County to make funding available to support smart growth-planning efforts in smaller jurisdictions seeking to build healthier communities for all residents.7
We were able to work with the Council of Governments to make sure that those residents who didn’t speak English ... had an environment that was open to them. And so we worked with them [the council] to make sure that there was [verbal and document] translation at the meetingsHIA practitioner in Kern and Fresno counties
Evaluating the HIA
Involving a range of stakeholders in the HIA encouraged decision-makers to consider the potential health implications of their SCS plans and future decisions. Since the completion of the HIAs in 2014, the HIA team has had ongoing conversations about equitable development at the regional and state levels with both counties’ planning organizations in order to elevate the needs of key populations in both counties.8
The HIA team’s work also led to increased communication and stronger relationships within and among government agencies across the region. County officials used the results to inform a decision made by the California Air Resources Board to ensure that dollars from the California Climate Investments Program—which sells carbon offsets to businesses—would be used for projects to reduce air pollution in lower-income communities.9 Furthering these reductions may help improve air quality and related health outcomes in Fresno, Kern, and similar communities.
Equitable bus service in the Bay Area
Transportation influences public health through, for example, road safety, pollution from vehicle emissions, and access to goods and services.10 People in low-income communities often face barriers to adequate transportation, such as affordability, service reliability, and quality, which can affect people’s ability to maintain employment or access important services such as health care.11
In 2012, the Alameda County Public Health Department partnered with 16 community and advocacy organizations to conduct an HIA on health impacts of cuts to bus service and fare increases on transit-dependent bus riders.12 Alameda County is located in the San Francisco Bay Area, which comprises nine ethnically and economically diverse counties, all with varying forms of transportation. The county’s bus operator, AC Transit, is one of the Bay Area’s largest and serves a higher percentage of people of color and from low-income households than the other systems in the region.
The HIA sought to inform the Regional Transportation Plan (RTP), the transportation component of Plan Bay Area, a long-range transportation, land-use, and housing plan approved by the Metropolitan Transportation Commission (MTC) and the Association of Bay Area Governments in July 2013. The RTP provides guidance on land-use investments and the region’s sustainable community strategy and directs the allocation of close to $300 billion in transportation funding across the region.
The department formed an advisory committee for the HIA, comprising public health, environmental, and transit organizations, as well as residents of Alameda County, which helped define the scope of the analysis, develop research questions and methods, collect data, and set priorities for the recommendations. The methodology included a review of published literature, an analysis of rider surveys, and interviews and focus groups with Alameda County residents.
The HIA focused on how the level of transit funding allocated in the RTP would affect the health of transitdependent bus riders in the county, particularly low-income individuals, people of color, youth, seniors, and riders with disabilities.13 These populations are often the most dependent on public transportation and therefore disproportionately affected by transit policies and programs.14
HIA recommendations
Based on the findings, the HIA team recommended that the MTC increase funding for bus services, assess the feasibility of a regional discounted transit pass program for low-income riders, and expand data collection efforts to include rider-experience and service-condition indicators, such as wait time, crowding, and travel time.15
Evaluating the HIA
The HIA engaged transit-dependent residents and other community members in the process, including having them participate in data collection, on the advisory committee, and in the development of the recommendations. Through this process, the assessment generated primary data on transit access and affordability in the county and helped decision-makers understand the perspectives and experiences of transit-dependent riders.
The findings demonstrated that buses are essential to meeting people’s basic needs, such as getting to work and school every day, and data from the focus groups showed the trade-offs that residents would have to make if fares were increased. Although the final Plan Bay Area did not include an increase in transit operations funding, the MTC did approve two important amendments, including a commitment to secure more funding for transit operations. In addition, AC Transit decided to forgo a bus fare increase scheduled for November 2013.
The HIA team conducted a stakeholder evaluation to measure satisfaction with its engagement efforts, which found that participants were pleased with their involvement in shaping the research design, scope, and prioritization of data. However, in the focus group for this review, some community stakeholders indicated that their input could have been better incorporated in the targeted dissemination and outreach to decision-makers during the reporting phase.
The team encountered several challenges related to engagement, including sustaining relationships among the large number of stakeholders, compressing the activities into the grant and decision-making timelines, and facilitating participation among certain groups, such as people with disabilities and non-English speakers. Additionally, tensions emerged between public agency and community partners regarding the risk of research bias.
Despite these challenges, the HIA helped the health department forge strong relationships with new community partners, build local capacity to use HIA, and provide a robust sample of primary data and compelling findings that informed the RTP and related work.
High school career academies for Oakland youth
The link between education and health is well-documented. Significant disparities in educational attainment exist across racial and ethnic groups and are strongly mediated by such factors as family poverty, local school funding and resources, and teacher experience.16 In spring 2013, Youth UpRising launched an HIA to inform the Oakland Unified School District’s plan to design and implement a second career academy at Castlemont High School to improve schoolwide academic achievement.17 Career academies, also known as learning academies, offer students smaller classes with college-preparatory or career-specific curricula.18
In the Castlemont community, which is located in Oakland, many families—and 35 percent of residents under 18—live below the poverty line.19 At the time of the HIA, 41 percent of adults older than 25 in the community had not graduated from high school, and more than half had dropped out before completing the ninth grade.20
To address community health disparities linked to educational inequities, Youth UpRising—a nonprofit organization committed to transforming the East Oakland community by developing youth leaders and improving the systems that shape their lives—organized a stakeholder work group of education and health agencies. That group, in turn, determined that an HIA would add value to the decision-making process regarding the new career academy. Youth UpRising then formed a group of five student researchers from the high school to lead the HIA under the direction of organization staff. After participating in an HIA training, the youth researchers developed an initial scope for the HIA that was finalized with the work group. The final scope focused on how the learning academies’ impact on social support, high school graduation, employment, and income may influence health.
The HIA ultimately included a literature review, one focus group with community residents, and eight interviews with stakeholders from the health and education fields. After data collection, the team participated in two retreats where the youth analyzed qualitative data and identified common themes from the interviews.
Scoping the HIA was a tremendously powerful tool to help not just put a health lens on all of these different issues but to really serve youth development. And if you really are concerned about long-term sustainable health impacts on communities, then why not involve the people who are going to be there when those impacts are realized?HIA practitioner in Oakland
HIA recommendations
Based on the findings, the HIA recommended strategies to facilitate job opportunities for students, such as offering a local tax credit to businesses that provide learning academy students with work experience through jobs or internships and ensuring that Castlemont’s career-specific curricula prepare students for success in the labor market. The HIA also recommended continuing to engage students in the high school’s decision-making processes by creating a youth council to provide ongoing feedback to teachers and involving students in evaluations of the quality and impact of the school.
Evaluating the HIA
Youth UpRising used findings and recommendations from the HIA to apply for and secure funding to add two new charter schools. Supporting youth to conduct the HIA empowered them to be a factor in decision-making that affects their lives and the Castlemont community, rather than leaving the authority entirely with the school district. The students were able to set the research questions and priority areas for the HIA, which, in turn, informed the Oakland Unified School District’s design of the new career academy at Castlemont High School.
This first-of-its-kind youth-led effort presented unique challenges for the HIA process, particularly with stakeholder engagement. For instance, school schedules took precedence over HIA activities, so the larger team had to be flexible when scheduling project meetings. Additionally, students were participating in training related to research methods, writing, community outreach, public health, and HIA while the data collection and analysis were underway, which meant each component of the HIA required more time.
Data from this evaluation of the HIA suggest that the systematic yet flexible approach of the Youth UpRising staff allowed the students’ learning to drive the process. As with other HIAs, competing priorities, employment shifts, and time constraints led to some instances of leadership turnover within key stakeholder groups, disrupting cohesion among those with knowledge of and commitment to the HIA.
Transit passes for youth in Los Angeles County
Providing public transportation to students has been an increasingly popular strategy among state and local municipalities to bolster school attendance.21 These efforts have the potential to improve health outcomes because education is an important determinant of health; high school completion can lead to higher-paying jobs and more stable income that in turn can affect access to other resources such as healthy food and safe communities.22 The design and implementation of public transportation programs for students vary in terms of the amount and types of fare covered (e.g., buses and metro-rail), age restrictions, and permissions for weekday and weekend usage. For instance, New York City provides free or reduced-price transit passes when schools are in session for students living a certain distance from their schools.23 Portland, Oregon, in contrast, does not restrict passes based on proximity but offers them only to high school students.24
Los Angeles has a diverse metro-rail, subway, and bus system provided by both county- and city-level transit agencies, the largest of which is the County Metropolitan Transportation Authority (MTA). Although the MTA offered reduced-price transit passes for students, some county leaders believed that costs still remained a barrier to school attendance. In spring 2013, the Los Angeles County Education Coordinating Council (ECC), which seeks to raise educational achievement of youth in the county’s foster and probation systems, passed a resolution in support of a recommendation from its School Attendance Taskforce that free transit passes be provided to all students in the county. The task force is a collaboration among the county’s mental health, social services, educational, legal, probation, and public health agencies and community-based organizations.
After passage of the resolution, the Los Angeles County Department of Public Health conducted an HIA to examine the potential health effects of the free transit pass proposal and to provide evidence to the public and local government on this issue. The HIA focused on how providing free transit passes might affect school attendance, fare evasion citations issued to young people, and school funding. It also considered possible effects on traffic volume and congestion, injuries, opportunities for physical activity, freedom and mobility for youth, and the relationship between these factors and health.25
The HIA used three primary data collection methods: literature review, secondary data analysis, and key informant interviews. The literature review examined research questions regarding how youth get to and from school and the costs and short- and long-term health impacts of providing free transit passes to students. The team then analyzed data from secondary sources to estimate the potential economic impacts of the resolution, including costs associated with lost fare revenue and increased transit ridership; economic gains for schools from reduced absences; and benefits to the community from lower emissions, increased disposable income for families, and decreased contact between youth and families and the justice system. Finally, the team conducted interviews with transportation and education experts to learn about other free or reduced-cost transit programs across the country.
We as a health field need to be more humble and not always put health at the center of the agenda. And go into collaboration seeking to understand what [our partners’] priorities are and what they want to work on.HIA practitioner in Los Angeles
The HIA team prioritized equity throughout the HIA process by using data to demonstrate different populations’ reliance on public transit, focusing on ways the resolution might affect the most transit-dependent groups, and engaging a range of sectors and stakeholders. The engagement component was driven, in large part, by the task force, which facilitated interagency collaboration. Participating in the task force helped the health department uncover and understand the priorities of other agencies involved, which, in turn, helped it identify shared objectives.
HIA recommendations
The HIA generated several recommendations, including to explore partnership opportunities between Los Angeles County transportation agencies and school districts to help increase student attendance, assess alternative options to expand existing discount-fare programs, and convene a multidisciplinary work group to discuss how the program could be cost-effectively implemented.
The ECC presented the HIA findings and recommendations for reducing transit barriers to educational achievement for youth to the MTA board during discussions of fare increases. Although a free transit pass program was not implemented, the board decided to freeze student fares while raising the base transit fare for all other riders by 17 percent, from $1.50 to $1.75.26
Evaluating the HIA
The HIA team successfully gathered a broad range of data that demonstrated the correlation among transportation barriers (including affordability), truancy, access to education, and health and solidified a trusting partnership with the task force. In interviews, the HIA practitioners described the challenge of conducting an HIA on a polarized issue that had to simultaneously consider the impediments students face in getting to school and transit agencies’ need to generate revenue. The HIA ultimately ensured that diverse stakeholder views informed the decision-making process, and presented a balanced account of the potential costs and benefits of the resolution.
Findings from the evaluation
Promoting community health
Involving stakeholders in decisions that affect them may lead to increased self-esteem and confidence, improved social relationships, and a greater sense of empowerment, which in turn can result in positive health outcomes, such as better mental health.27 This evaluation sought to gauge the effectiveness of these HIAs in delivering similar benefits, as well as broader local or regional impacts. The early evidence suggests some impact, including the provision of additional funds for charter schools that stemmed from the Youth UpRising HIA; the Fresno Council of Governments’ decision to conduct a needs assessment of transportation deficiencies and health outcomes; the holding flat of bus fares in Alameda County; and the continuation of discounted transit passes for Los Angeles County students. These actions will probably have effects on health, but it is too soon to document them.
Community perspective
Capturing stakeholders’ experiences of participating in the HIAs and with the outcomes of the decisions under consideration was another key objective of this evaluation. In the focus groups, stakeholders described whether and how HIA teams were intentional and effective in their engagement efforts. They expressed that when the HIA teams prioritized outreach and community involvement, stakeholders were more likely to participate. Teams that were able to strike a balance between leveraging residents’ perspectives and the other core tenets of HIA did so by including stakeholders throughout the process or by taking an integrated approach in which community members were part of the team conducting the HIA. The Youth UpRising HIA is an example of the latter, where the students affected by the school district’s decisions received training and led the HIA process. The HIAs administered by the Departments of Health in Alameda and Los Angeles counties involved community stakeholders in specific stages, particularly the data collection, and provided them with opportunities to share their personal experiences with decision-makers.
A common theme that emerged from this evaluation was that engagement is demanding in terms of the time and energy required and the capacity necessary to respond directly to concerns raised through engagement. One HIA team member observed that, “Sometimes community stakeholders say things we don’t want to hear, and it is hard on us to figure out how to deal with that.”
Several members of HIA teams mentioned that sustaining engagement throughout the entire process was a challenge that was made more difficult by personnel turnover and competing schedules and responsibilities. Another issue was defining the scope and scale of the affected populations. Some assessed decisions that would affect specific groups or geographic areas, which made identifying relevant stakeholders easier for the HIA teams compared with those examining less defined populations or places.
Capacity
This evaluation asked the teams about their use of the technical assistance and grant funds, their partnerships, and their capacity to conduct future HIAs. One HIA team used grant funds to pay an outside organization to lead community workshops on data collection and analysis for community members. Some respondents commented that it was helpful to have money available to retain experts, especially people with HIA experience. Youth UpRising used the technical assistance service to bring in a special provider to train the teenage members of the team and the community participants. Other teams mentioned that the benefit of technical assistance was limited by logistical issues, such as the decision-making timeline, but that they were able to translate the available tools and resources to meet the needs of their projects.
The process of conducting HIAs affected both the teams and the community stakeholders. For example, the members of the Youth UpRising HIA team gained research and presentation skills and had the opportunity to inform their school’s priorities. Other teams developed the knowledge and skills to engage stakeholders in future work and learned how to bring a health perspective to decision-making.
As a result of the HIAs, teams developed stronger relationships with and among organizations and sectors. For example, participants in the Alameda County HIA described how the process resulted in stakeholder groups, such as transit agencies, reaching out to the health department for support on other decisions to ensure that their work better promotes health and engages the community. Similarly, the HIA team in Fresno and Kern counties facilitated a dialogue between community partners and local agencies that led to tangible improvements to infrastructure, such as revamped sidewalks and enhanced community connectivity. And as a result of its work on the Los Angeles HIA, that team changed the practices of its organization to make consideration of the values and priorities of other sectors a routine part of its review of proposed decisions.
Incorporating health into decision-making
This evaluation found that the HIAs generally made decision-makers aware of the connections between the proposals being assessed and impacts on health in effective and compelling ways and that the final decisions and actions taken typically reflected that understanding. For example, in the wake of the Fresno and Kern counties HIAs, decision-makers are hosting hearings on how best to ensure that California Climate Investments Program dollars support planning in disadvantaged communities. Some interviewees commented that the effects of the HIA on the decision could have been greater had a range of dissemination strategies been employed and that it was not enough just to send out a report. Follow-up outreach, presentations, and advocacy strategies were needed to ensure that HIA findings were considered by decision-makers and accessible to community members. Respondents observed that when reports were sent out without follow-up with decision-makers and stakeholders, possibly because of resource, timing, and capacity constraints, the potential influence of the recommendations and reports was curtailed. In some cases, dissemination and impact were complicated by reports that illuminated costs, which made the recommendations less appealing for decision-makers.
Lessons learned
The difficulties that teams encountered in conducting the HIAs were similar to those faced by HIA practitioners generally, and many centered on trade-offs between full execution of each of the Minimum Elements and Practice Standards for HIA, which describe the essential components of assessments and provide guidance for effective HIA practice. For example, respondents said that although collaborating with and hearing from stakeholders is valuable, it required additional effort because of schedules, feedback that complicated the research questions and scope of work, and a lack of shared expectations or underlying knowledge. They also reported that effectively communicating technical and complex issues to community members in a manner that would allow for informed participation and maintenance of an objective analytical lens was sometimes difficult.
Identifying the appropriate group to communicate findings and recommendations was another challenge. One HIA team from the public health sector was well-positioned to conduct the scientific research and identify recommendations, and intentionally structured the process to keep its analysis distinct from any advocacy related to the assessed decision. Some teams said that effective cross-sector collaboration emerged when they were able to manage expectations, establish buy-in around a shared understanding of the goals, and find the appropriate role for the public health perspective.
In addition, although monitoring and evaluation is one of the six steps of HIA, it is often not included or thoroughly completed in the process because it falls outside the time frame or funding for the finalized assessment and sometimes is beyond the skill set of the team. For these and other reasons, some teams did not continue to monitor or evaluate their HIAs. For example, one organization shifted its focus so that the HIA topic was no longer a priority, and another team, without having the HIA process to convene community stakeholders, ceased its engagement and lost the opportunity to monitor implementation of the recommendations.
Overall, the teams viewed HIA as a valuable tool and expressed interest in doing future assessments, but they noted the importance of determining early whether HIA is appropriate for the proposed decision. They also raised concerns about conducting future HIAs and whether effective collaboration among such diverse affected parties could occur only with the opportunity presented by the grant. Some respondents said that because HIA needs to be timely, rigorous, and flexible, before conducting an assessment, practitioners should carefully consider several factors, including availability of adequate funding and other resources, timing of the HIA relative to the decision it will inform, and the political context. HIA is not the only tool available, and alternative assessments and community engagement approaches may be more appropriate for bringing health considerations to the decision-making process when HIA is not feasible or suitable.
To facilitate a community-led process and position the most suitable organization to communicate the recommendations, one team suggested having partners co-lead the HIA with public health professionals providing technical assistance or data support and engaging funders that are committed to broad stakeholder outreach. In the end, they said, it comes down to capacity, defined as having an understanding of the approach; the ability to collect, analyze, and communicate data; and sufficient resources and relationships to engage community stakeholders.
Conclusion
Findings from this evaluation suggest that HIAs can be a powerful tool for ensuring that the perspectives and expertise of community stakeholders are heard and considered during decision-making. Because of the Youth UpRising HIA, teens were able to present findings to decision-makers, inform people about the research they conducted, and affect the final decision. In Alameda and Los Angeles counties, the HIA process allowed a team to look comprehensively at the issue of transportation using rigorous data and to present compelling information to decision-makers that highlighted the reliance of certain populations on public transit. The Fresno and Kern counties HIAs helped residents participate in local planning meetings and shape the development of a sustainable community strategy that better reflects their needs.
The lessons learned indicate that, to maximize the potential of HIA, funders and lead organizations must consider what resources and capacity are needed to achieve the level of community stakeholder engagement that is required to attain impact.
Methods
The Health Impact Project used a case study approach involving multiple methods that included document review, semistructured interviews, and focus groups. The evaluators reviewed existing products from each HIA team, including the completed report and process and impact evaluations submitted as grant deliverables. Using a semistructured interview guide, the team conducted in-depth telephone interviews with at least two members from each assessment team for a total of 10 HIA team members across the four projects. The Health Impact Project also coordinated with the teams to recruit community stakeholders and conducted interviews and focus groups with nine of them. The interviews and focus groups were recorded, transcribed, and entered into NVivo, a qualitative data management and analysis software. The Health Impact Project created a coding book based on the research questions, coded each of the transcripts, and summarized key themes using NVivo. The Johns Hopkins Bloomberg School of Public Health Institutional Review Board approved the qualitative data collection procedures.
Endnotes
- Erika Cheng and David Kindig, “Disparities in Premature Mortality Between High- and Low-Income US Counties,” Preventing Chronic Disease 9 (2012): 110120, http://dx.doi.org/10.5888/pcd9.110120; Leadership Counsel for Justice and Accountability, Health Impact Assessment: California’s SB 375 and Its Impact on Fresno County’s Disadvantaged Unincorporated Communities and Low Income Urban Neighborhoods (2014), http://media.wix.com/ugd/53e872_674db7f1158a4234bd8eae5c51942071.pdf; and Leadership Counsel for Justice and Accountability, Health Impact Assessment: California’s SB 375 and Its Impact on Kern County’s Disadvantaged Unincorporated Communities and Low Income Urban Neighborhoods (2014), http://media.wix.com/ugd/53e872_7fc08d007aa14880939bf0cd77fcda66.pdf.
- American Lung Association, State of the Air 2016, http://www.lung.org/assets/documents/healthy-air/state-of-the-air/sota-2016-full.pdf.
- California Environmental Protection Agency, Air Resources Board, Air Quality and Land Use Handbook: A Community Health Perspective (2005), 8–11, http://www.arb.ca.gov/ch/handbook.pdf; W. James Gauderman et al., “Effect of Exposure to Traffic on Lung Development From 10 to 18 Years of Age: A Cohort Study,” Lancet, no. 9561 (2007): 571–77, doi:10.1016/S0140-6736(07)60037-3; and Ying-Ying Meng et al., “Living Near Heavy Traffic Increases Asthma Severity,” UCLA Center for Health Policy Research (2006), http://healthpolicy.ucla.edu/publications/Documents/PDF/Living Near%20Heavy%20Traffic%20Increases%20Asthma%20Severity.pdf.
- According to the U.S. Department of Health and Human Services, equity is the “attainment of the highest level of health for all people. Achieving health equity requires valuing everyone equally with focused and ongoing societal efforts to address avoidable inequalities, historical and contemporary injustices, and the elimination of health and health care disparities.” U.S. Department of Health and Human Services, “Glossary of Terms,” accessed June 24, 2016, http://www.minorityhealth.hhs.gov/npa/templates/browse.aspx?lvl=1&lvlid=34.
- California Environmental Protection Agency, Air Resources Board, “Sustainable Communities,” accessed June 1, 2016, http://www.arb.ca.gov/cc/sb375/sb375.htm.
- As defined by the U.S. Department of Transportation’s Federal Transit Administration, “A Metropolitan Planning Organization is the policy board of an organization created and designated to carry out the metropolitan transportation planning process.” Federal Transit Administration, “Metropolitan Planning Organization (MPO),” accessed June 20, 2016, https://www.transit.dot.gov/regulations-and-guidance/transportation-planning/metropolitan-planning-organization. A Regional Transportation Plan is defined by the California Department of Transportation as “a Federal and State mandated planning document prepared by Metropolitan Planning Organizations and Regional Transportation Plan Agencies. The plan describes existing and projected transportation needs, conditions, and financing affecting all modes [of transportation] within a 20-year horizon.” California Department of Transportation, Draft 2015 Metropolitan Planning Organization Regional Transportation Plan Review Report (February 2016), http://www.dot.ca.gov/hq/tpp/offices/orip/rtp/draft-rtp-review-rpt.pdf.
- Smart growth solutions are defined by Smart Growth America as “solutions [that] support thriving businesses and jobs, provide more options for how people get around and make it more affordable to live near work and the grocery store. Our coalition works with communities to fight sprawl and save money.” Smart Growth America, “About Us,” accessed May 9, 2016, http://www.smartgrowthamerica.org/about/.
- As defined by PolicyLink, equitable development is an “approach to creating healthy, vibrant, communities of opportunity. Equitable outcomes come about when smart, intentional strategies are put in place to ensure that everyone can participate in and benefit from decisions that shape their neighborhoods and regions.” PolicyLink, “Equity Tools,” accessed June, 24, 2016, http://www.policylink.org/equity-tools/equitable-development-toolkit/about-toolkit.
- The California Climate Investments Program is a part of California’s Cap and Trade Program, which is a strategy to reduce pollution, and is supported by credits purchased by companies that produce large amounts of greenhouse gas emissions. Center for Climate and Energy Solutions, “California Cap-and-Trade Program Summary” (2014), http://www.c2es.org/docUploads/calif-cap-trade-01-14.pdf.
- U.S. Department of Transportation, Research and Innovative Technology Administration, John A. Volpe National Transportation Systems Center, Metropolitan Area Transportation Planning for Healthy Communities (2012), https://www.planning.dot.gov/documents/ Volpe_FHWA_MPOHealth_12122012.pdf.
- Urban Design 4 Health Inc., “The Hidden Health Costs of Transportation” (March 2010), http://apha.org/~/media/files/pdf/topics/transport/ hidden_health_costs_of_transportation_backgrounder.ashx.
- Alameda County Public Health Department, Getting on Board for Health: A Health Impact Assessment of Bus Funding and Access (May 2013), http://www.acphd.org/media/308854/transithia.pdf; and Metropolitan Transportation Commission, Statistical Summary of Bay Area Transit Operators: Fiscal Years 2009-10 Through 2013-14 (July 2015), http://mtc.ca.gov/sites/default/files/StatSumm_2014.pdf.
- Alameda County Public Health Department, Getting on Board for Health; and American Public Transportation Association, A Profile of Public Transportation Passenger Demographics and Travel Characteristics Reported in On-Board Surveys (May 2007), http://www.apta.com/resources/statistics/Documents/ transit_passenger_characteristics_text_5_29_2007.pdf.
- John Pucher and John L. Renne, “Socioeconomics of Urban Travel: Evidence From the 2001 NHTS,” Transportation Quarterly 57, no. 3 (2003): 49–77, http://www.sharetheroad.ca/pdf/(Pucher)-Socioeconomics-of-Urban-Travel.pdf.
- Alameda County Public Health Department, Getting on Board for Health.
- William Jeynes, “A Meta-Analysis on the Factors That Best Reduce the Achievement Gap,” Education and Urban Society, 47, no. 5 (2015): 523–54, doi:10.1177/0013124514529155; Center for American Progress, Speaking of Salaries, What It Will Take to Get Qualified, Effective Teachers in All Communities (May 2011), https://cdn.americanprogress.org/wp-content/uploads/issues/2011/05/pdf/teacher_salary.pdf; and Caroline Ratcliffe and Signe-Mary McKernan, Child Poverty and Its Lasting Consequence, Low-Income Working Families Paper 21 (September 2012), The Urban Institute, http://www.urban.org/sites/default/files/alfresco/publication-pdfs/412659-Child-Poverty-and-Its-Lasting-Consequence.PDF.
- Youth UpRising, Career Pathway at Castlemont High School: Youth-Driven Health Impact Assessment (January 2014), //www.pewtrusts.org/~/media/assets/external-sites/health-impact-project/youth-uprising-2014-castlemont-high-school-report.pdf?la=en.
- Betsy Brand, “High School Career Academies: A 40-Year Proven Model for Improving College and Career Readiness,” National Career Academy Coalition (November 2009) http://www.aypf.org/documents/092409CareerAcademiesPolicyPaper.pdf.
- Youth UpRising, Career Pathway at Castlemont High School.
- Ibid.
- Los Angeles County Department of Public Health, “The Potential Costs and Benefits of Providing Free Public Transportation Passes to Students in Los Angeles County” (April 2014), http://publichealth.lacounty.gov/plan/docs/hia/04.22.2014addendum.pdf.
- Robert Wood Johnson Foundation, “Why Does Education Matter So Much to Health?” updated March 2013, http://www.rwjf.org/en/library/research/2012/12/why-does-education-matter-so-much-to-health-.html.
- New York City Department of Education, Office of Pupil Transportation, “Student MetroCards,” accessed May 9, 2016, http://www.optnyc.org/ServicesAndEligibility/metrocards.htm.
- TriMet, “Youth Tickets and Passes,” accessed May 9, 2016, https://trimet.org/fares/youth.htm.
- Los Angeles County Department of Public Health, “The Potential Costs and Benefits of Providing Free Public Transportation Passes to Students in Los Angeles County.”
- Laura J. Nelson, “MTA Board Votes to Increase Fares on Metro Bus and Rail Lines,” Los Angeles Times, May 22, 2014, http://www.latimes.com/local/lanow/la-me-ln-metro-fare-hike-20140522-story.html.
- Pamela Attree et al., “The Experience of Community Engagement for Individuals: A Rapid Review of Evidence,” Health and Social Care in the Community 19, no. 3 (2011): 250–60, doi:10.1111/j.1365-2524.2010.00976.x.


America’s Overdose Crisis
Sign up for our five-email course explaining the overdose crisis in America, the state of treatment access, and ways to improve care
Sign up

This video is hosted by YouTube. In order to view it, you must consent to the use of “Marketing Cookies” by updating your preferences in the Cookie Settings link below. View on YouTube
This video is hosted by YouTube. In order to view it, you must consent to the use of “Marketing Cookies” by updating your preferences in the Cookie Settings link below. View on YouTube


Kids Score Skate Park Using Health Data






