State Prison Health Care Spending
QUICK SUMMARY
This report finds that state spending on prisoner health care increased from fiscal 2007 to 2011, but began trending downward from its peak in 2009. Nationwide, prison health care spending totaled $7.7 billion in fiscal 2011, down from a peak of $8.2 billion in fiscal 2009. In a majority of states, correctional health care spending and per-inmate health care spending peaked before fiscal 2011. But a steadily aging prison population is a primary challenge that threatens to drive costs back up. The share of older inmates rose in all but two of the 42 states that submitted prisoner age data. States where older inmates represented a relatively large share of the total prisoner population tended to incur higher per-inmate health care spending.
OVERVIEW
Health care and corrections have emerged as fiscal pressure points for states in recent years as rapid spending growth in each area has competed for scarce revenue. Not surprisingly, the intersection of these two spheres— health care for prison inmates—also has experienced a ramp-up, reaching nearly $8 billion in 2011.
Under the landmark 1976 Estelle v. Gamble decision, the U.S. Supreme Court affirmed that prisoners have a constitutional right to adequate medical attention and concluded that the Eighth Amendment is violated when corrections officials display “deliberate indifference” to an inmate’s medical needs.1 The manner in which states manage prison health care services that meet these legal requirements affects not only inmates’ health, but also the public’s health and safety and taxpayers’ total corrections bill. Effectively treating inmates’ physical and mental illnesses, including substance use disorders, improves their well-being and can reduce the likelihood that they will commit new crimes or violate probation once released.2
The State Health Care Spending Project previously examined cost data from 44 states* and found that prison health care spending increased dramatically from fiscal year 2001 to 2008. However, new data from a survey of budget and finance staff officials in each state’s department of corrections, administered by The Pew Charitable Trusts and the Vera Institute of Justice, show that some states may be reversing this trend.
This report examines the factors driving costs by analyzing new data on all 50 states’ prison health care spending from fiscal 2007 to 2011.† It also describes a variety of promising strategies that states are using to manage spending, including the use of telehealth technology, improved management of health services contractors, Medicaid financing, and medical or geriatric parole.
The project’s analysis of the survey data yielded the following findings:
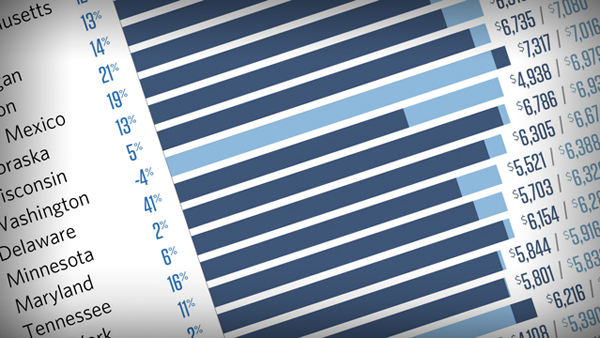
- Correctional health care spending rose in 41 states from fiscal 2007 to 2011, with median growth of 13 percent, after adjusting for inflation.
- Per-inmate health care spending also rose in 39 states over the period, with a median growth of 10 percent.
- In a majority of states, however, total spending and per-inmate spending peaked before fiscal 2011.
Nationwide, prison health care spending totaled $7.7 billion in fiscal 2011, down from a peak of $8.2 billion in fiscal 2009. The downturn in spending was due, in part, to a reduction in state prison populations. - From fiscal 2007 to 2011, the share of older inmates—who typically require more expensive care—rose in all but two of the 42 states that submitted prisoner age data.‡ Not surprisingly, states where older inmates represented a relatively large share of the total prisoner population tended to incur higher per-inmate health care spending.
As states work to manage prison health care expenditures, a downturn in spending was a positive development as long as it did not come at the expense of access to quality care. But states continue to face a variety of challenges that threaten to drive costs back up. Chief among these is a steadily aging prison population.
Data from the survey can provide state decision-makers with information to assess both their own state’s spending—over time and compared with other states—as well as cost-containment initiatives underway from fiscal 2007 to 2011. Officials in all 50 states were willing to respond to the survey and supply spending information, which is a strong indication of their eagerness to make peer comparisons and address spending in a data-driven fashion.
- * The source of these data was the Bureau of Justice Statistics.
- 1 William J. Rold, "Thirty Years After Estelle v. Gamble: A Legal Retrospective," Journal of Correctional Health Care 14, no. 1 (2008): 11–20, doi:10.1177/1078345807309616.
- 2 Steve Aos, Marna Miller, and Elizabeth Drake, "Evidence-Based Adult Corrections Programs: What Works and What Does Not," Washington State Institute for Public Policy (2006), http://www.wsipp.wa.gov/rptfiles/06-01-1201.pdf; Elizabeth Maier, Peter Wicklund, and Max Schlueter, “Evidence-Based Initiatives to Reduce Recidivism,” Vermont Center for Justice Research (December 2011), http://66.147.244.94/~vcjrorg/reports/reportscrimjust/reports/ebiredrecid_files/DOCRR%20LitRev%20Report.pdf; Fred Osher et al., "Adults With Behavioral Health Needs Under Correctional Supervision: A Shared Framework for Reducing Recidivism and Promoting Recovery," Council of State Governments Justice Center (2012), http://www.asca.net/system/assets/attachments/4908/9.27.12_Behavioral_Framework_v6_full.pdf?1348755628; David Mancuso and Barbara E.M. Felver, "Providing Chemical Dependency Treatment to Low-Income Adults Results in Significant Public Safety Benefits," Washington State Department of Social and Health Services Research and Data Analysis Division (February 2009), http://www.dshs.wa.gov/pdf/ms/rda/research/11/140.pdf; and Melissa Ford Shah et al., "The Persistent Benefits of Providing Chemical Dependency Treatment to Low-Income Adults," Washington State Department of Social and Health Services Research and Data Analysis Division (November 2009), http://www.dshs.wa.gov/pdf/ms/rda/research/4/79.pdf.
10 %
The growth of per-inmate spending on prison health care over five years before peaking in 37 states before 2011.
Learn MoreADDITIONAL RESOURCES

Article
Fact Sheet




