Strategies to Encourage Safe Methadone Use in Medicaid
State policies aim to decrease risk of overdose

Overview
Methadone is a long-acting opioid that is predominantly used to mitigate withdrawal symptoms in individuals with opioid use disorder (OUD). However, beginning in the mid-1990s, use of the drug for the treatment of noncancer pain increased. While methadone can provide effective pain relief, its pharmacologic properties present safety challenges when it is used for chronic pain.1 Methadone pain relief lasts four to eight hours, but the drug’s effects on the heart and lungs continue for a longer period of time.2 Patients may therefore take more of the drug to control pain before the heart- and lung-related effects of the original dose have stopped, thus putting themselves at risk. When taken too often, methadone can cause life-threatening respiratory depression and heart rhythm or heart rate abnormalities.3 These effects can result in an overdose or death.
While the drug is not widely used for pain management—it accounts for only about 1 percent of all opioid prescriptions—it is associated with roughly 23 percent of opioid-related overdose deaths.4 Federal and state agencies have sought to reduce the risk of harm associated with the use of methadone for pain, and many state Medicaid programs have implemented strategies to help achieve this goal. These include the use of public and private payer policies that define parameters for the safe use of prescriptions, also known as medication-use policies.
Methadone for pain: Federal and state agencies address safety concerns
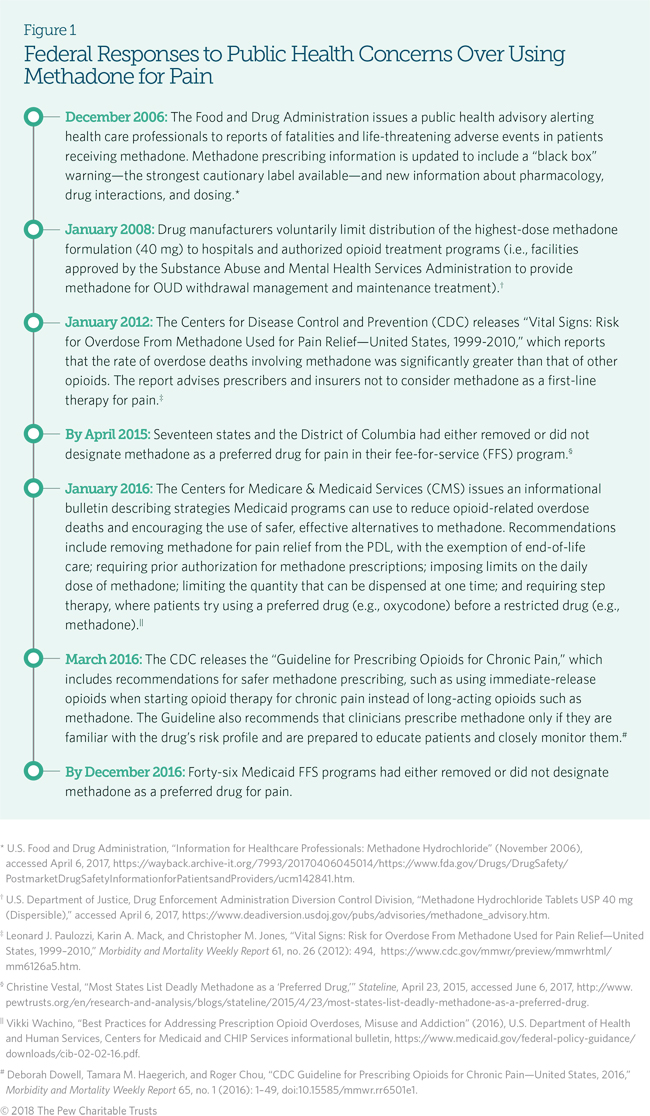
Federal agencies charged with addressing public health and safety recognize that prescribing methadone for pain increases the risk of overdose and death, and have taken steps to reduce prescribing of the drug. (See Figure 1.) At the state level, Medicaid agencies also have a strong interest in reducing the risk of harm from methadone and other opioids. Medicaid agencies utilize a variety of strategies to encourage or discourage the use of a specific drug. Medicaid preferred drug lists (PDLs) are one strategy that identifies medications eligible for payment without prior authorization, which requires approval from the Medicaid agency or managed care plan.5
Historically, many Medicaid agencies have considered methadone a preferred medication for the treatment of chronic pain because of the drug’s effectiveness, potency, and lower cost compared with other opioid pain medications.6 More broadly, studies that analyzed prescribing data between 2000 and 2012 found that Medicaid beneficiaries were prescribed opioids at twice the rate of individuals with other insurance coverage, and were three to six times more likely than them to experience an overdose.7 Medicaid programs’ removal of methadone from the PDL is one strategy to promote safe use of the drug; other tools include limits on the dose and quantity of methadone that a patient can receive in an effort to improve the safety of prescribing methadone for pain. Medicaid programs in Massachusetts, Oregon, Washington, and West Virginia are among those that have successfully implemented these strategies to more safely prescribe methadone for pain and minimize risks to patients who use the drug.
Medicaid strategies to promote safe and effective drug use
States employ a variety of approaches to promote safe and cost-effective medication use, such as designating a drug as “non-preferred,” requiring prior authorizations, and enacting dose limits. Often, Medicaid agencies use multiple strategies simultaneously in an effort to encourage or discourage the prescribing of specific drugs.
Non-preferred designation and prior authorization
A pharmacy and therapeutics (P&T) committee or drug utilization review (DUR) board meets periodically throughout the year to evaluate medications for preferred status and inclusion on the Medicaid PDL. These multidisciplinary bodies comprise practicing health care professionals, primarily physicians and pharmacists. The meetings may be open to the public, and provide consumers opportunity for input.
Through this process, Medicaid agencies designate drugs as “preferred” or “non-preferred,” with non-preferred drugs generally requiring prior authorization—which means prescribers must obtain approval from Medicaid staff to use a drug for a specific patient.8 These designations typically apply to Medicaid FFS programs, in which health care providers are reimbursed for each service that is performed and billed, such as office visits, diagnostic tests, and procedures. In many states, Medicaid managed care organizations (MCOs) set their own PDL. MCOs deliver health care services to their beneficiaries through contracted arrangements between Medicaid agencies and MCOs that agree to accept a set payment per member per month for all contracted services.
Medicaid agencies determine prior authorization criteria using evidence-based standards, which may mean providers must take specific actions to obtain approval before a drug is paid for, such as documenting the therapy goals or assessing a patient’s risk of substance use disorder (SUD). P&T committees or DUR boards evaluate requests for prior authorization against evidence-based recommendations for patient selection, drug dosage, drug administration, and duration of therapy to ensure safety and optimize patient outcomes. The prior authorization process is intended to encourage safe use of the most clinically effective and least expensive medication possible for a given condition.9 States can use prior authorization requirements to limit prescribing a drug to specific indications, such as reserving methadone use for pain to patients with a cancer diagnosis.10 Emerging evidence from CDC indicates an association between non-preferred designation of methadone for pain on the PDL and lower rates of methadone-related overdose deaths.11
Dose limits
Medicaid agencies may restrict a specific drug’s maximum daily dose, whether it is designated preferred or non-preferred. Known as a dose limit, the strategy ensures that dosing does not exceed thresholds associated with safe, appropriate use of any medication. Some Medicaid programs have imposed limits on the daily dose of opioids, including methadone, that can be prescribed. The 2016 CDC Guideline recommends a maximum daily opioid dose of 90 morphine milligram equivalents (MMEs), a measure that compares an opioid dose’s potency to morphine. That recommended dose equates to approximately 20 mg of methadone per day.12
Other strategies
Additional approaches implemented to reduce the harms associated with prescribing methadone for pain include:13
- Educating Medicaid providers about safe methadone prescribing practices, including the importance of screening patients for known risk factors (e.g., contraindicated medications, mental health conditions) and the need for ongoing monitoring.
- Setting quantity limits, which—in order to promote the medication’s safe and appropriate use—restrict the amount of a drug that may be prescribed or dispensed during a specific time frame.
- Using step therapy, which requires trying a preferred drug first. The use of the restricted drug is authorized only if the patient does not respond to, or cannot tolerate, the preferred drug.
- Engaging in DUR processes to identify potentially inappropriate trends among prescribers that can be addressed through general education of all Medicaid prescribers or targeted education of individual ones.
Examples of states improving methadone use for pain
To better understand strategies for reducing methadone-related harms and encouraging the use of safer, effective alternatives for chronic pain, researchers from The Pew Charitable Trusts interviewed staff from Medicaid agencies in four states—Washington, Oregon, West Virginia, and Massachusetts. These states took steps between 2007 and 2015 to change methadone’s preferred status and educate prescribers, and encountered few, if any, barriers when implementing these changes.
Washington
In March 2007, Washington became the first state to release a guideline on opioid dosing for chronic, non-cancer pain.14 The guideline, which was developed by state officials in collaboration with practicing clinicians and pain researchers, was issued in response to a twelvefold increase in opioid-related overdose deaths in employees receiving workers’ compensation for work-related injuries. Between 1995 and 2002, roughly 72 percent of overdose deaths among workers’ compensation patients involved methadone.15 The guideline recommended that the total daily dose of opioids not be increased above 120 MMEs (roughly 30 mg of methadone) unless a patient demonstrated improved function and decreased pain, or had a consultation with a pain specialist.16
Public attention was drawn to the issue of methadone-related overdose deaths when the Legislature questioned Medicaid staff in response to a series of 2011 articles in The Seattle Times investigating the agency’s methadone coverage policy.17 The investigators found that while Medicaid recipients comprised only 8 percent of Washington’s adult population, they accounted for nearly half of the state’s methadone-related deaths. Following the articles and legislative questioning, the Washington State Health Care Authority—which administers both Medicaid and the Public Employees Benefits Board Program—sent a letter to Medicaid providers on the challenges of using methadone for pain, and contacted the top 20 prescribers of methadone to discuss appropriate use of the drug.
Recognizing that more could be done to improve safety, the DUR board in October 2015 approved removing methadone from the PDL. As of March 1, 2016, prior authorization is required unless a patient has cancer-related pain, has tried and failed all other generic long-acting opioids, is in hospice care, or was already stabilized on daily doses of methadone greater than 40 mg. The exemption for patients stable on high doses of methadone helped to alleviate concerns raised by experienced methadone prescribers, who noted the challenges associated with transitioning these patients to equipotent doses of other long-acting opioids. However, dose escalations for these patients require prior authorization. Meanwhile, patients who were being treated with doses of methadone under 40 mg as of March 1, 2016, were required to discontinue the drug and switch to a different long-acting opioid medication. The decision to impose prior authorization criteria was generally well accepted by prescribers.18
These changes, which apply to managed care plans and FFS patient populations, also apply to the state’s Public Employees Benefits Board Program and Department of Labor & Industries’ workers’ compensation program.
To support the March 2016 changes, in September 2017 the Washington State Health Care Authority began issuing feedback reports to providers identified as having patients who receive high doses of opioids. The reports allow providers to compare their prescribing patterns with those of their peers. In addition, the agency implemented a policy, effective Oct. 1, 2017, that limits the amount of opioids dispensed for acute pain.
Oregon
In 2010, Oregon’s Medicaid agency, the Oregon Health Plan, took a multistep approach to address safety concerns related to the use of methadone as a treatment for chronic pain. Overdose deaths caused by opioids, particularly methadone, had highlighted the need for action: In 2008, methadone accounted for one-third of the state’s deaths due to poisoning.19 In January 2010, the agency placed initial restrictions on methadone use, including prior authorization criteria for doses exceeding 100 mg per day; doses above that threshold would be approved only after ruling out risk factors, such as structural heart disease and a lack of previous prescriptions for methadone within the last month. Just over two years later, in April 2012, Oregon reduced the maximum allowable daily dose of methadone to 40 mg. If a patient’s daily dose exceeded that amount, the prescriber was asked to taper it down. Dose limits for new patients were also added, allowing them a maximum daily dosage of 20 mg of methadone.
In July 2013, in response to growing public health concerns surrounding methadone-related overdose deaths and national efforts to decrease the use of methadone for pain, the director of pharmacy programs for Medicaid’s oversight agency recommended the P&T committee designate methadone as non-preferred. Committee members agreed; the recommendation was approved the following month. In January 2014, methadone became non-preferred for the Medicaid FFS population, which represents 10 percent of the state’s Medicaid patient population. Because Oregon’s 16 coordinated care organizations function similarly to Medicaid managed care plans in other states, they were not required to make this change.
Finally, in July 2016, in response to the 2016 CDC Guideline, the state’s Medicaid program decreased the dose limit from 40 mg to 20 mg for all patients, including those stabilized on higher doses of methadone, with prior authorization for doses exceeding 20 mg granted to allow for the tapering of a patient’s dose.
Now, methadone can be prescribed in Oregon for pain treatment only if the following prior authorization criteria are met: (1) the drug is prescribed for an appropriate use (e.g., an FDA-approved indication); (2) it is prescribed for a covered condition; and (3) the total daily dose does not exceed 20 mg.
These changes in Oregon were associated with a decline in the Medicaid FFS population that was prescribed methadone for pain, with 0.5 percent of beneficiaries receiving the drug in 2012 and 0.2 percent in 2015.
West Virginia
In October 2013, West Virginia Medicaid was one of the first programs to classify methadone as non-preferred for pain. As a result, as of Jan. 1, 2014, providers had to receive prior authorization before prescribing methadone for any use, with the exception of a cancer diagnosis. This change was prompted by an independent family physician’s suggestion that Medicaid reclassify methadone for pain as non-preferred due to its risk profile, and concern that physicians with less experience prescribing the drug might interpret preferred designation to mean it was safe for unrestricted use, despite its long half-life and risk of respiratory depression. Local and national publicity on methadone-related deaths also influenced West Virginia’s P&T committee to vote unanimously to reclassify methadone as non-preferred. Any patient previously prescribed methadone for pain was permitted to continue use of the drug only after receiving approval from both West Virginia Medicaid’s medical director and the DUR pharmacist.
Following this policy change, West Virginia Medicaid notified all providers in writing of methadone’s non-preferred status for all Medicaid patients (FFS and managed care) and explained the rationale for the change.
According to state officials, reclassifying methadone as non-preferred resulted in decreased methadone prescribing, from roughly 22 percent in 2013 to 8 percent in 2016. These results caused the agency to consider establishing prescribing guidelines for other opioids.
The Medicaid agency has adopted the CDC Guideline, and also implemented Safe and Effective Management of Pain, a program targeted to prescribers with patients on long-term opioid therapy with doses exceeding 50 MME per day. The program encourages the use of non-opioid medications and other treatment modalities for chronic pain. If and when opioids are determined to be the most appropriate treatment for a patient’s pain, the program encourages prescribers to use the lowest possible dose, monitor the treatment’s effectiveness, and educate patients on the side effects of opioids and use of naloxone.
Massachusetts
MassHealth—the state’s Medicaid agency—addressed methadone prescribing in several ways, including provider education, prior authorization, and dose limits. Prompted by warnings from federal agencies about the overdose risk associated with the use of methadone for pain, MassHealth first convened a multidisciplinary, multiagency stakeholder meeting in September 2015 to discuss proposed changes to opioid prescribing and methadone use. The meeting included representatives from the Department of Public Health, the Bureau of Substance Abuse Services, treatment providers, pain specialists, addiction medicine specialists, and pharmacists, and provided MassHealth with an opportunity to gain buy-in to the proposed changes by sharing evidence on the safe prescribing of opioids, particularly methadone, and allowing participants to ask questions and voice concerns.
Following that meeting, MassHealth implemented a prior authorization requirement for patients who had not filled a methadone prescription in 60 out of the previous 90 days. The requirement, which went into effect in March 2016, exempted patients who were stabilized on methadone for pain. Requests for prior authorization are evaluated based on a number of criteria, such as whether the patient has already tried or is not a candidate for a different long-acting opioid.
Also in March 2016, MassHealth reduced the total daily dose limit for all opioids from 240 MMEs (approximately 60 mg of methadone) to 120 MMEs (approximately 30 mg of methadone). A consultation from a provider trained in the condition causing the patient’s pain (e.g., oncologist, rheumatologist) is required for patients to obtain doses that exceed 30 mg per day. This broadened the agency’s definition of a consulting provider to include other clinicians in addition to pain specialists, which helped alleviate prescriber concerns about an insufficient supply of pain specialists to conduct the consultation. The consultation must include a signed and dated patient–prescriber agreement for pain treatment with opioid medications, along with medical records documenting the treatment plan, including the rationale for high-dose methadone therapy and the history of titration to the current dose. Patients who were stable on methadone when these requirements went into effect in March 2016 were not subject to the prior authorization criteria, but were subject to the dose limit; any patient taking more than 30 mg of methadone had the dosage tapered down.
Medicaid managed care plans, which provide care for half of the state’s Medicaid beneficiaries, were required to mirror these drug policy changes.
A patient-prescriber opioid therapy agreement is a document outlining a patient’s responsibility to avoid improper use of opioids or other controlled substances. It includes policies on lost medication, refills, the use of urine drug screens, education about drug storage and disposal, and the provider’s responsibility to treat the patient with respect, answer questions, and provide contact information for use in case of emergency.*
* Commonwealth of Massachusetts, Department of Public Health, “Prescriber Guide to Interpreting Prescription Monitoring Program Data,” (2013), accessed June 29, 2017, http://www.mass.gov/eohhs/docs/dph/quality/ drugcontrol/prescriber-guide-interpreting-pmp-data.pdf.
Before the prior authorization requirement and dose limit went into effect, MassHealth sent a “Dear Prescriber” letter to Medicaid providers that highlighted the risks associated with high doses of opioids, and informed prescribers of the pending dose limits and prior authorization criteria for methadone.20 Pharmacists from MassHealth were available to answer prescriber questions.
MassHealth also took several steps to ease the process of changing the status of methadone for pain. For example, to alleviate some of the burden of prior authorization for providers treating a high number of patients with chronic pain whose treatment necessitates a dose increase, the agency allows for a one-time dose increase of up to 35 percent without prior authorization. Additionally, a longstanding clinical work group facilitated communication with MassHealth prescribers on prior authorization requirements and restrictions, and continues to meet every two weeks to discuss outlier cases (e.g., patients with high-dose opioid use).21 Members of the work group are responsible for oversight of all opioid analgesic use and follow-up with prescribers with complex patient cases to discuss clinically appropriate treatment options and care plans for those identified as being at high risk for overdose.
The changes led to decreased utilization of methadone for pain. Between September 2015 and February 2016, 577 beneficiaries were using methadone for pain with a median daily dose of 40 mg. Following the March 2016 policy changes adding prior authorization and dose limits, total use and the average dose of methadone for pain decreased; from May 2016 to October 2016, the total number of beneficiaries using methadone for pain declined 33 percent to 384, with the median daily dose reduced by 25 percent to 30 mg.
Conclusion
According to Medicaid programs that have implemented medication-use initiatives to improve the prescribing of methadone for pain, federal agencies’ increased focus on methadone and other opioid-related overdose deaths helped to facilitate policy changes. Decisions to implement policies that were more restrictive than existing practices were met with limited resistance from prescribers and other stakeholders. However, some Medicaid providers—especially clinicians experienced in treating pain and using methadone—were less immediately accepting of the prescribing restrictions. To address these concerns, Washington, Oregon, West Virginia, and Massachusetts underscored the importance of maintaining adequate methadone access for patients for whom it remains appropriate (e.g., patients stabilized on high doses of the medication). Provider education and communication helped states achieve acceptance of these policies.
Medicaid programs that have yet to implement safety mechanisms for improving the safe prescribing of methadone for pain have cited a lack of resources, competing priorities, or other pressing public health concerns as primary barriers.22 However, in Washington, Oregon, West Virginia, and Massachusetts, implementing medication-use policy changes for methadone use for pain was a successful undertaking with minimal effort. States that have not yet taken steps to improve the safety of methadone use for chronic pain should consider implementing medication-use policies and other strategies for doing so.
Endnotes
- Ilene B. Anderson and Thomas E. Kearney, “Use of Methadone,” Western Journal of Medicine 172, no. 1 (2000): 43-46,https://www.ncbi. nlm.nih.gov/pmc/articles/PMC1070723/.
- U.S. Food and Drug Administration, “Information for Healthcare Professionals: Methadone Hydrochloride” (November 2006), accessed April 6, 2017, https://wayback.archive-it.org/7993/20170406045014/https://www.fda.gov/Drugs/DrugSafety/ PostmarketDrugSafetyInformationforPatientsandProviders/ucm142841.htm.
- Ibid.
- Mark Faul, Michele Bohm, and Caleb Alexander, “Methadone Prescribing and Overdose and the Association With Medicaid Preferred Drug List Policies—United States, 2007–2014,” Morbidity and Mortality Weekly Report 66, no. 12 (2017): 321, doi:10.15585/mmwr. mm6612a2.
- Vikki Wachino, “Best Practices for Addressing Prescription Opioid Overdoses, Misuse and Addiction” (2016), U.S. Department of Health and Human Services, Centers for Medicaid and CHIP Services informational bulletin, https://www.medicaid.gov/federal-policy-guidance/ downloads/cib-02-02-16.pdf; Faul, Bohm, and Alexander, “Methadone Prescribing,” 321.
- Leonard J. Paulozzi, Karin A. Mack, and Christopher M. Jones, “Vital Signs: Risk for Overdose From Methadone Used for Pain Relief— United States, 1999–2010,” Morbidity and Mortality Weekly Report 61, no. 26 (2012): 494, https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6126a5.htm.
- Jennifer Braden et al., “Trends in Use of Opioids by Non-Cancer Pain Type 2000-2005 Among Arkansas Medicaid and HealthCore Enrollees,” The Journal of Pain 9, no. 11 (2008): 1026-1035, https://doi.org/10.1016/j.jpain.2008.06.002; Centers for Disease Control and Prevention, “Poisoning Deaths Involving Opioid Analgesics—New York State, 2003-2012,” Morbidity and Mortality Weekly Report 64, no. 14 (2015): 377-380, https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6414a2.htm; Centers for Disease Control and Prevention, “Overdose Deaths Involving Prescription Opioids Among Medicaid Enrollees—Washington, 2004-2007,” Morbidity and Mortality Weekly Report 58, no. 42 (2009): 1171-1175, https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5842a1.htm.
- Wachino, “Best Practices”; Faul, Bohm, and Alexander, “Methadone Prescribing,” 321.
- Wachino, “Best Practices”; Academy of Managed Care Pharmacy, “Concepts in Managed Care Pharmacy: Prior Authorization” (2012), http://www.amcp.org/prior_authorization/.
- Wachino, “Best Practices.”
- Wachino, “Best Practices”; Faul, Bohm, and Alexander, “Methadone Prescribing,” 322.
- Deborah Dowell, Tamara M. Haegerich, and Roger Chou, “CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016,” Morbidity and Mortality Weekly Report 65, no. 1 (2016): 16, doi:10.15585/mmwr.rr6501e1; Centers for Disease Control and Prevention, “CDC Guideline for Prescribing Opioids for Chronic Pain,” fact sheet, accessed June 6, 2017, https://www.cdc.gov/drugoverdose/pdf/guidelines_at-a-glance-a.pdf.
- Wachino, “Best Practices.”
- Mark D. Sullivan et al., “Trends in Opioid Dosing Among Washington State Medicaid Patients Before and After Opioid Dosing Guideline Implementation,” The Journal of Pain 17, no. 5 (2016): 562, doi:10.1016/j.jpain.2015.12.018.
- Gary M. Franklin et al., “Opioid Dosing Trends and Mortality in Washington State Workers’ Compensation, 1996–2002,” American Journal of Industrial Medicine 48, no. 2 (2005): 91–99, http://dx.doi.org/10.1002/ajim.20191.
- Gary Franklin et al., “A Comprehensive Approach to Address the Prescription Opioid Epidemic in Washington State: Milestones and Lessons Learned,” American Journal of Public Health 105, no. 3 (2015): 464, doi:10.2105/AJPH.2014.302367.
- The Seattle Times, “Seattle Times Methadone Investigation Wins Pulitzer Prize” (April 16, 2012, updated April 17, 2012), accessed April 6, 2017, http://www.seattletimes.com/seattle-news/seattle-times-methadone-investigation-wins-pulitzer-prize/.
- Charissa Fotinos, Washington State Health Care Authority, pers. comm., August 2017.
- Oregon State University, College of Pharmacy, “Oregon Drug Use Review Board,” accessed June 21, 2017, http://s3.amazonaws.com/zanran_storage/pharmacy.oregonstate.edu/ ContentPages/2439023210.pdf.
- Paul L. Jeffrey, “Updated Opioid High Dose Limits” (2016), accessed June 21, 2017, http://www.mass.gov/eohhs/docs/masshealth/pharmacy/opioid-letter-high-dose-limits.pdf
- Maria M. Garcia et al., “Implementation of an Opioid Management Initiative by a State Medicaid Program,” Journal of Managed Care Pharmacy 20, no. 5 (2014): 447–54, http://www.jmcp.org/doi/pdf/10.18553/jmcp.2014.20.5.447.
- The Pew Charitable Trusts, “Informal Conversations With Medicaid Staff,” unpublished data.


America’s Overdose Crisis
Sign up for our five-email course explaining the overdose crisis in America, the state of treatment access, and ways to improve care
Sign up


Use of Methadone for Pain Declines in U.S.
Efforts by Medicaid, others to encourage safe prescribing practices may have helped reduce risks


The Use of Methadone for Pain by Medicaid Patients
An examination of prescribing patterns and drug use policies
ADDITIONAL RESOURCES

Podcast








